My Role
Competitive analysis
Accessibility design
As one of four UX designers in Group B4, I contributed across the full project arc:
We followed a human-centred design process across five stages, using each phase to ground our decisions in real user needs rather than assumptions.
The gap across all three: no single app combined structured progress tracking, community, professional access, and personalised AI support. That combination became Clink’s core proposition.
🧩 Solution Highlights
🧠 Conversational AI
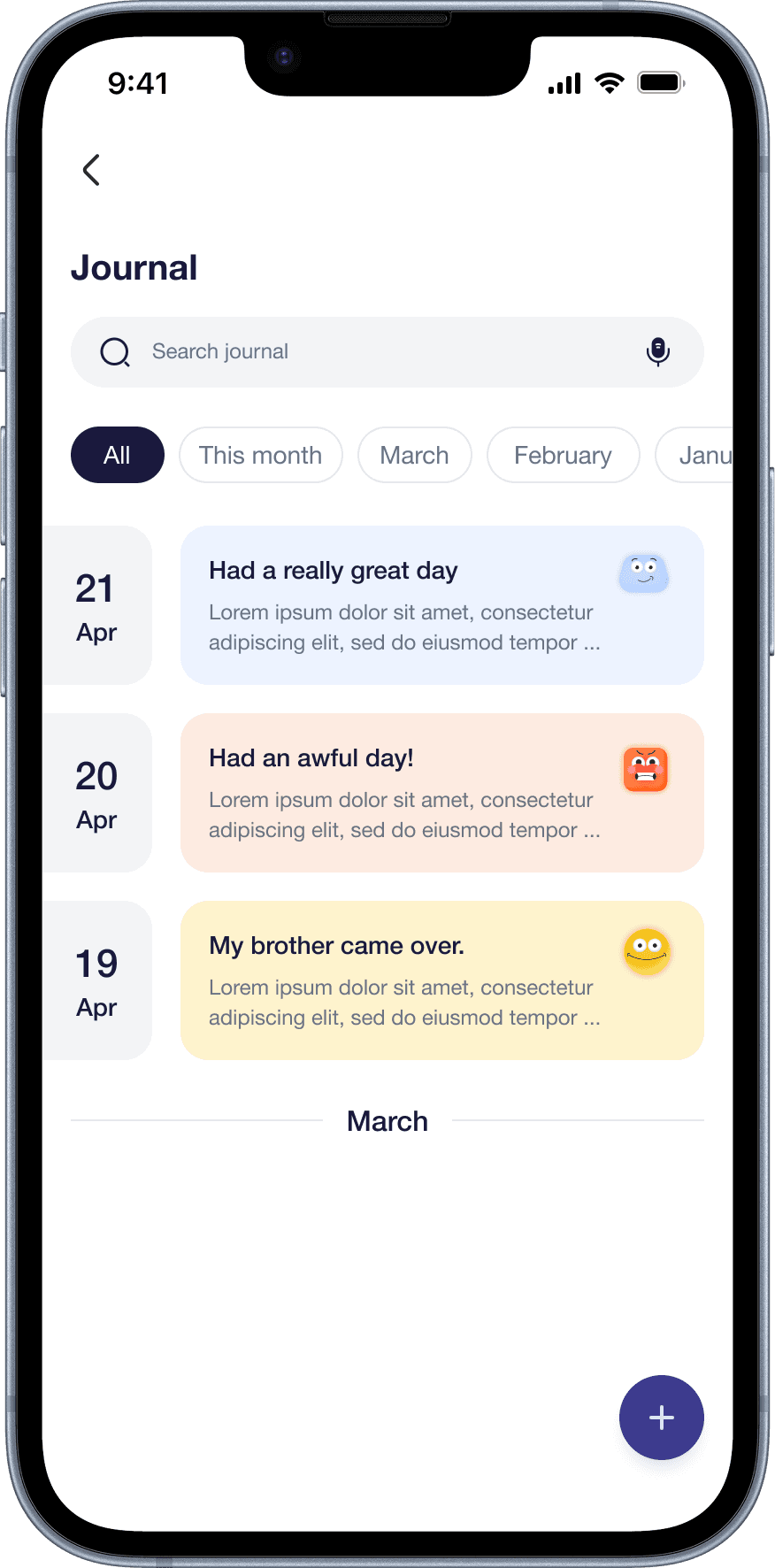
Our survey revealed that most previous quit attempts relied on distraction and lifestyle changes rather than structured support. The conversational AI was designed to fill that gap, providing a private, non-judgemental space for users to reflect on cravings, log how they’re feeling, and receive personalised guidance.
Crucially, it doubles as the onboarding mechanism: instead of a form, users answer questions through a conversation, making the experience feel human from the first interaction.



📈 Personalised Dashboard
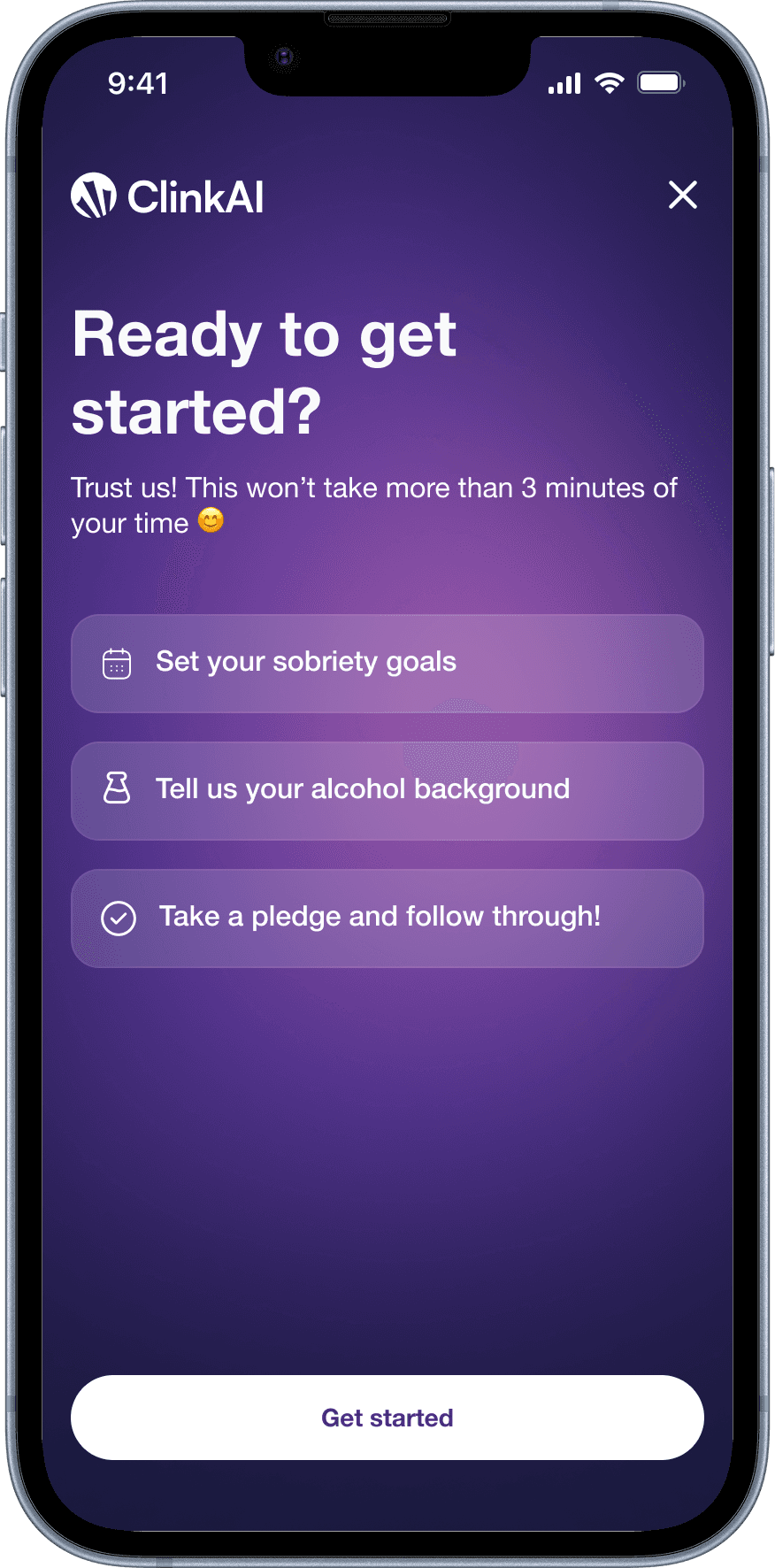
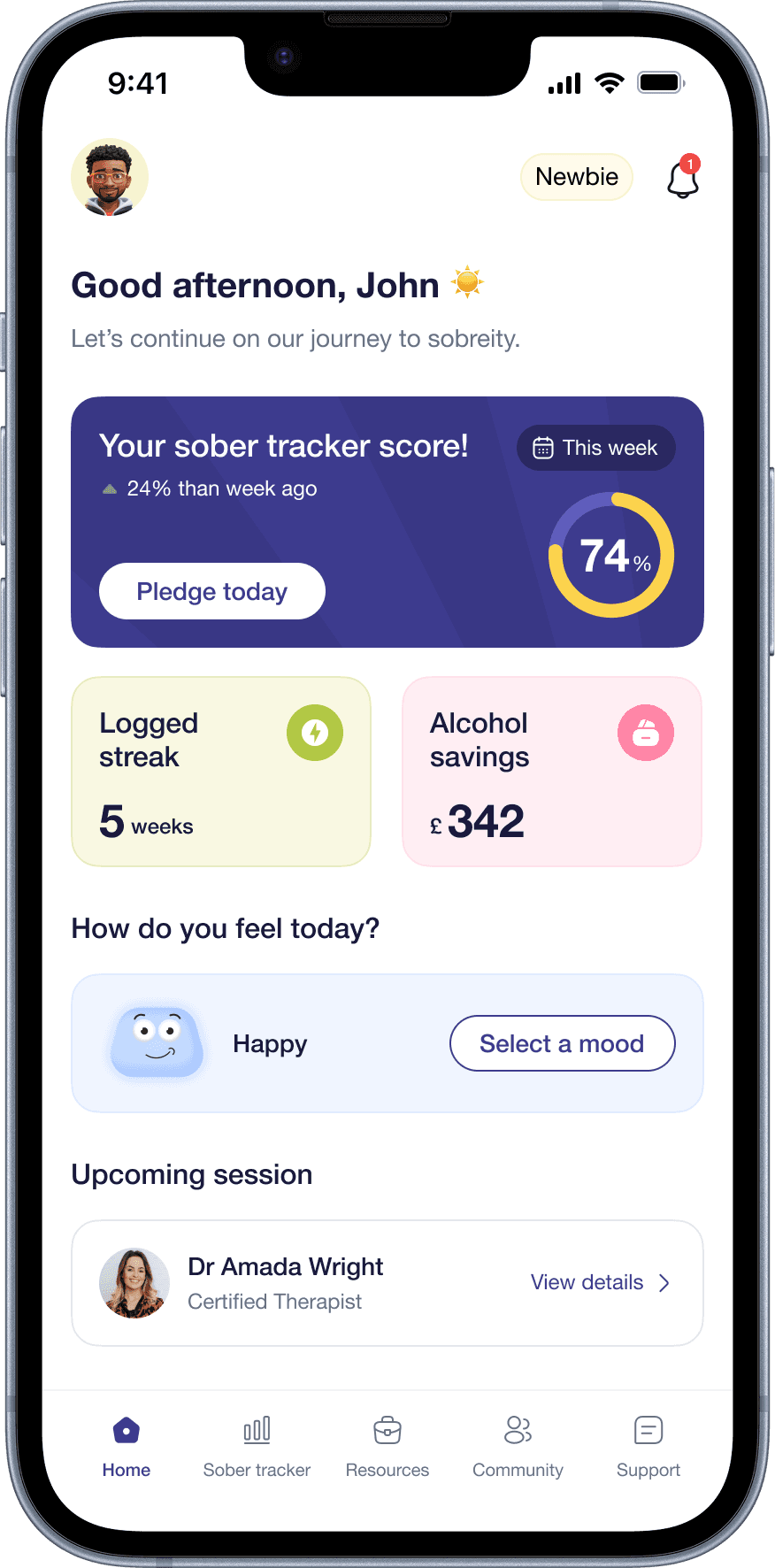
One of the clearest signals from research was that users wanted to track progress but existing apps tracked only what they drank, not how they were changing. The Clink dashboard surfaces a sober tracker score, a logged streak, alcohol savings in pounds, and a mood check-in on a single screen.
Every metric was chosen because it answers a question users actually care about: Am I improving? What am I gaining? How do I feel today?


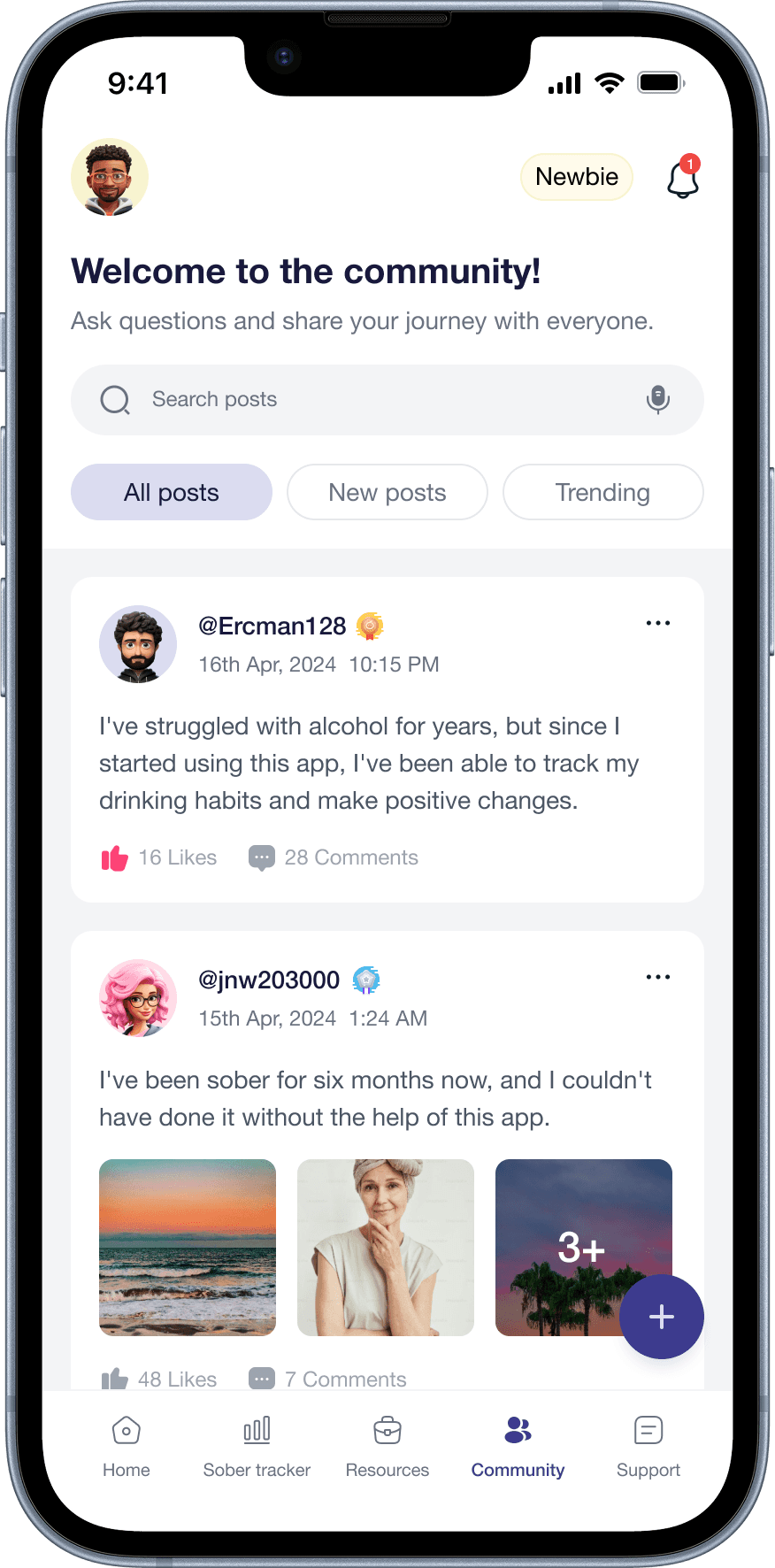
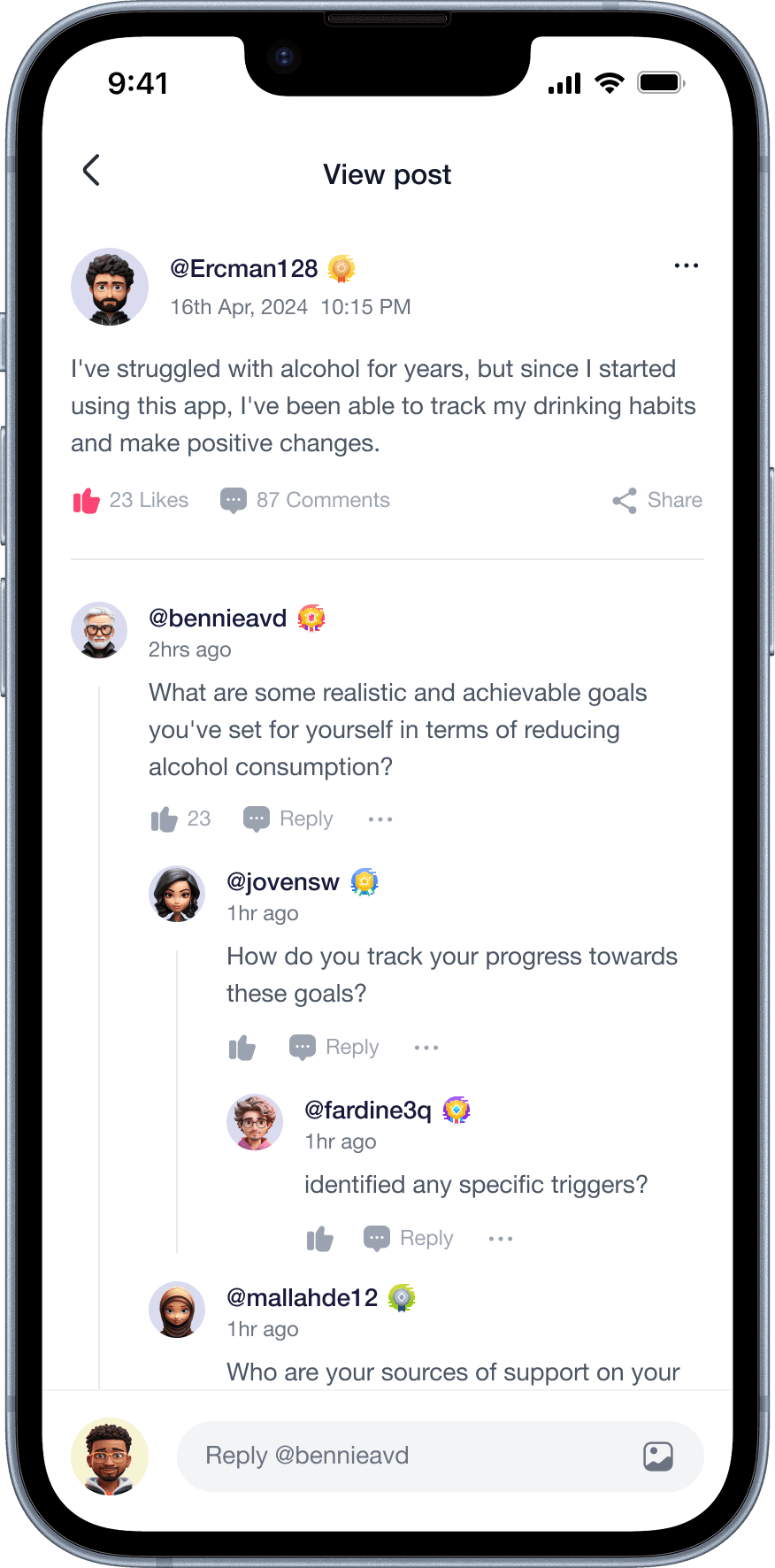
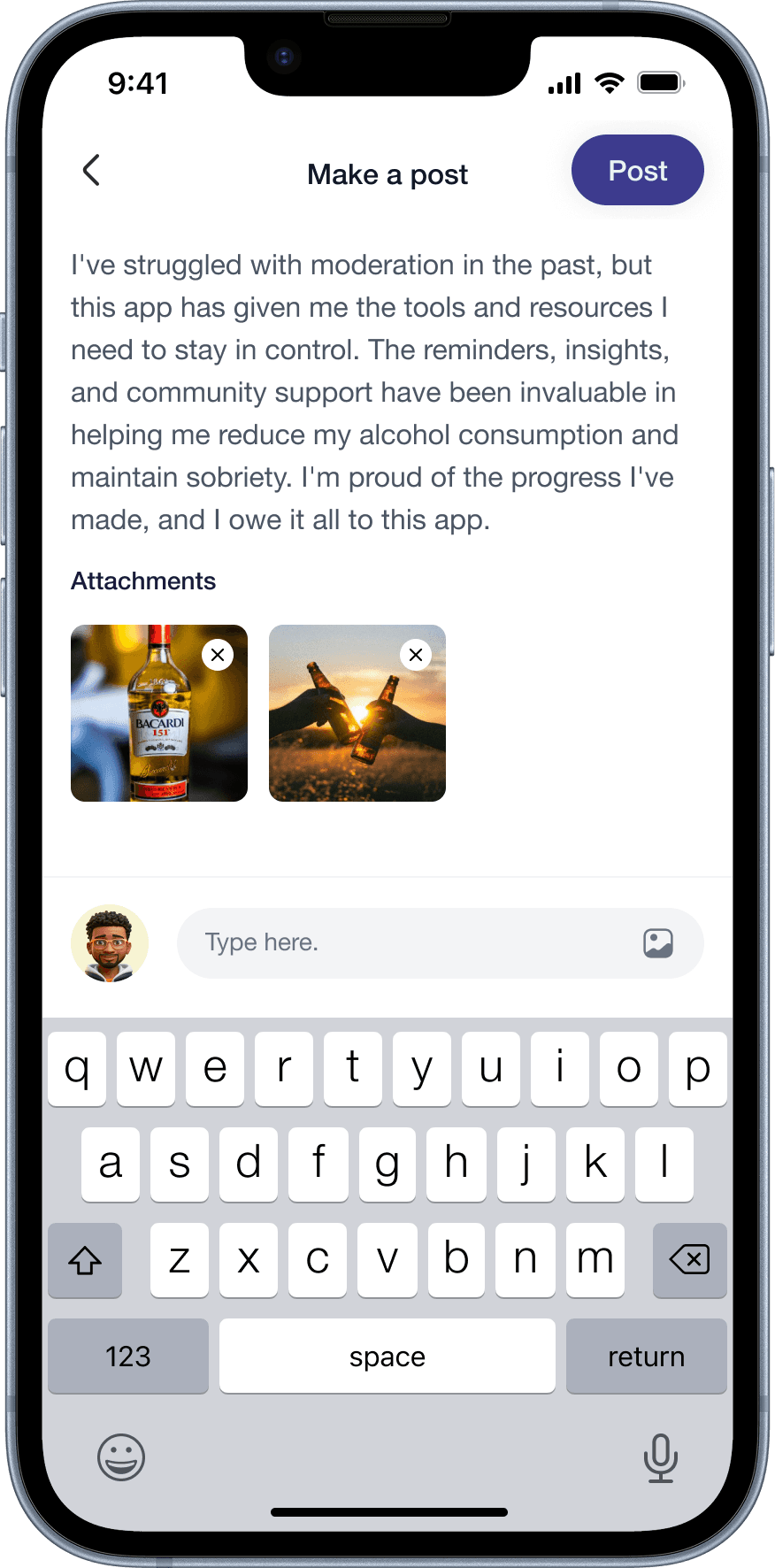
🫂 Anonymous Support Community
50% of survey respondents said they’d be interested in connecting with others trying to quit.
But stigma was the primary barrier to seeking help in the first place. We designed the community as fully anonymous by default, with no direct messaging (a deliberate choice to address the safety weakness we identified in Sober Sidekick).
Users can post, comment, and offer empathy badges, but within a moderated, safe environment.

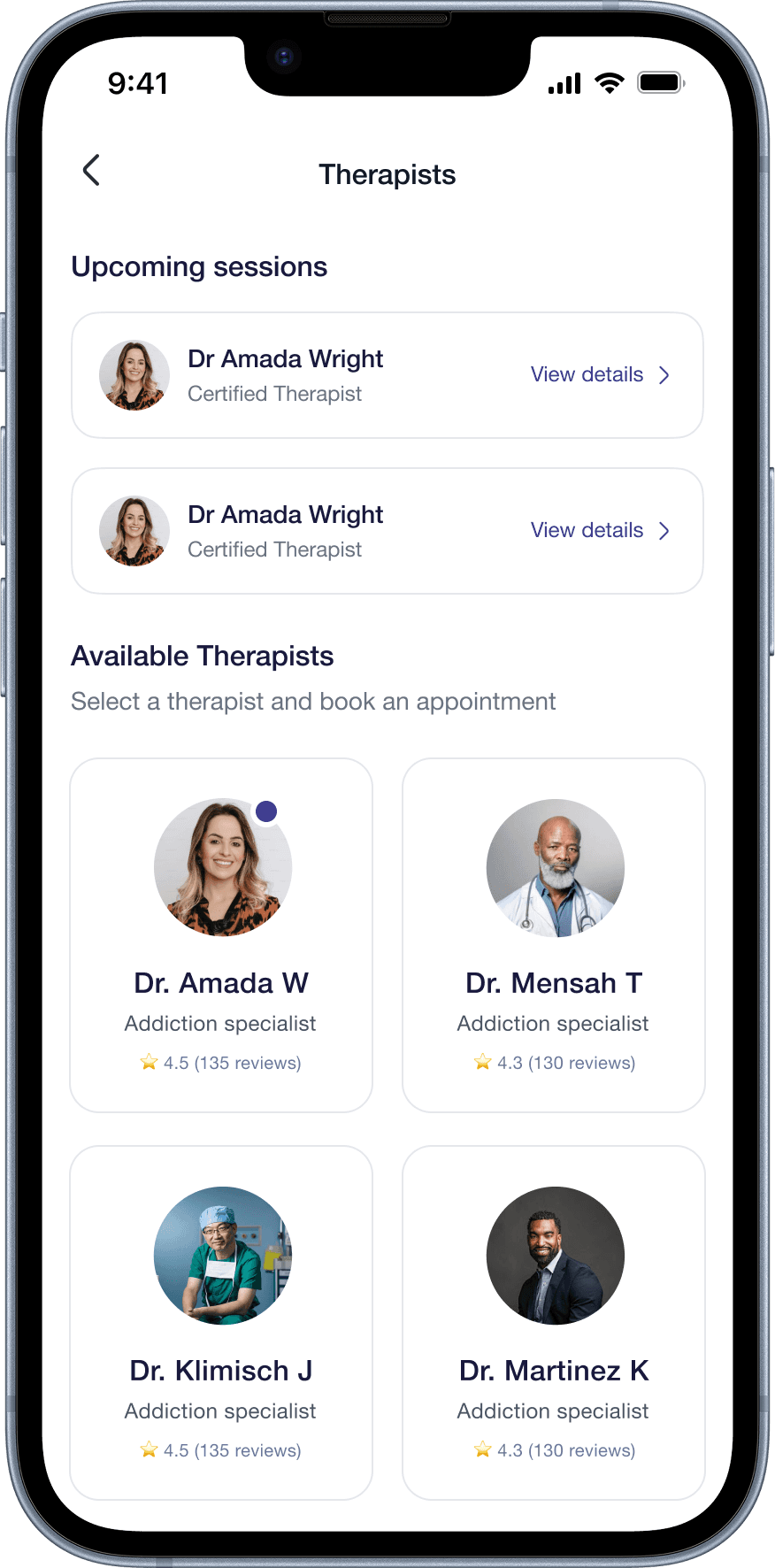
🧑⚕️ Therapist Access
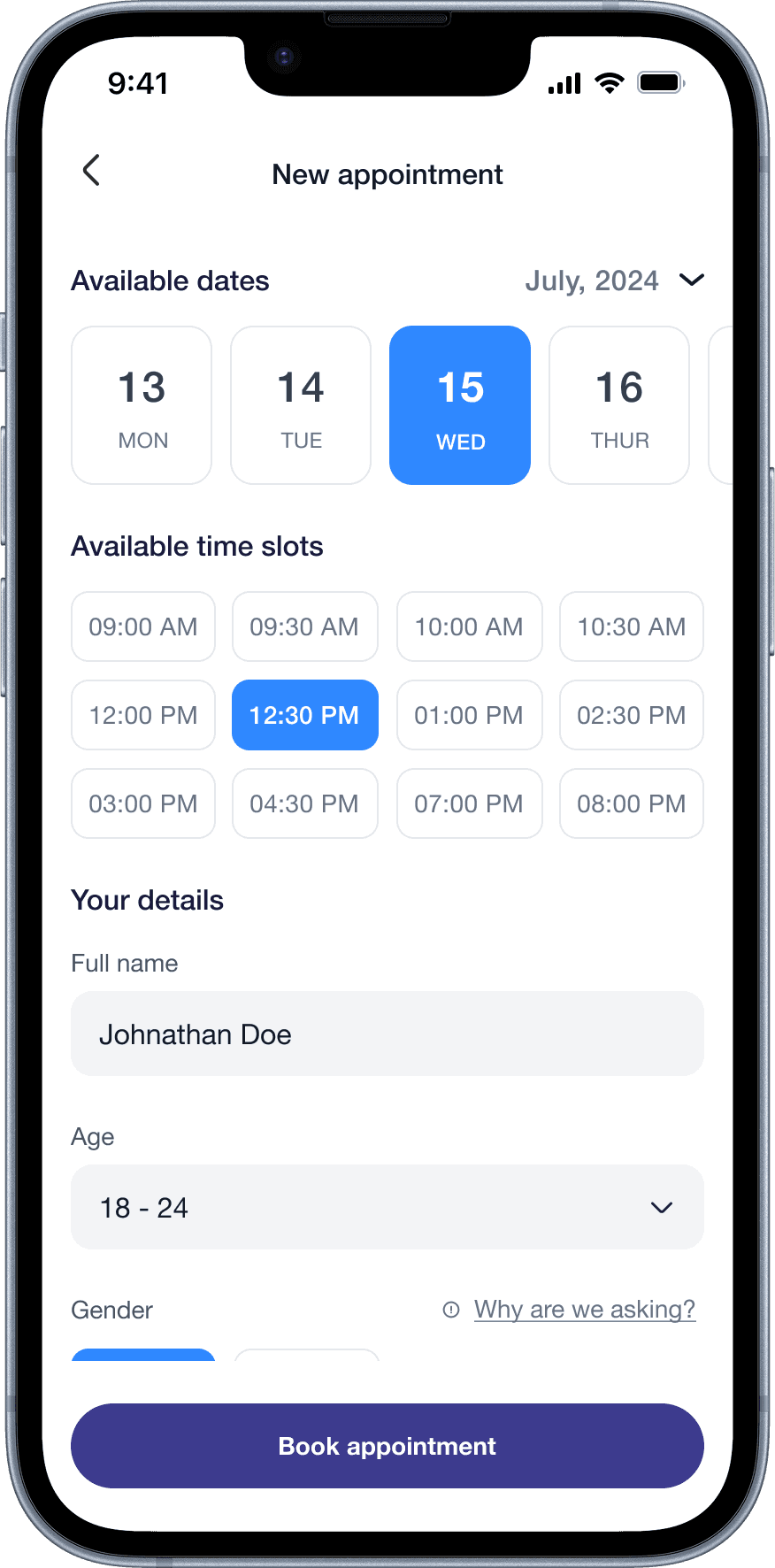
The competitive audit showed no existing app made it easy to connect to a licensed therapist within the same experience. Clink’s therapist module lets users browse certified therapists, view their specialisations and patient counts, and book appointments directly with calendar integration and email confirmation.
The design deliberately shows therapist credibility signals (years of experience, patient count, reviews) before the booking step, addressing the trust barrier our research surfaced.


♿ Inclusive UX for Users with Disabilities
We designed explicitly for users with physical and sensory disabilities. William (paraplegia) and Maria (visual impairment) were full personas with distinct goals, habits, and pain points, not afterthoughts.
For Maria, this meant designing with screen reader compatibility, voice-guided navigation, and accessible content formats in mind. This pushed us to question every design decision: does this work if you can’t see it? Does this work if you can’t use your hands?



📊 The Results




💡 What I Learned